Using Disaggregated Data to Uncover Asian American Breastfeeding Initiation Gaps
Samantha Liv
2026 Council of State and Territorial Epidemiologists (CSTE) Annual Conference • Boston, MA
Background
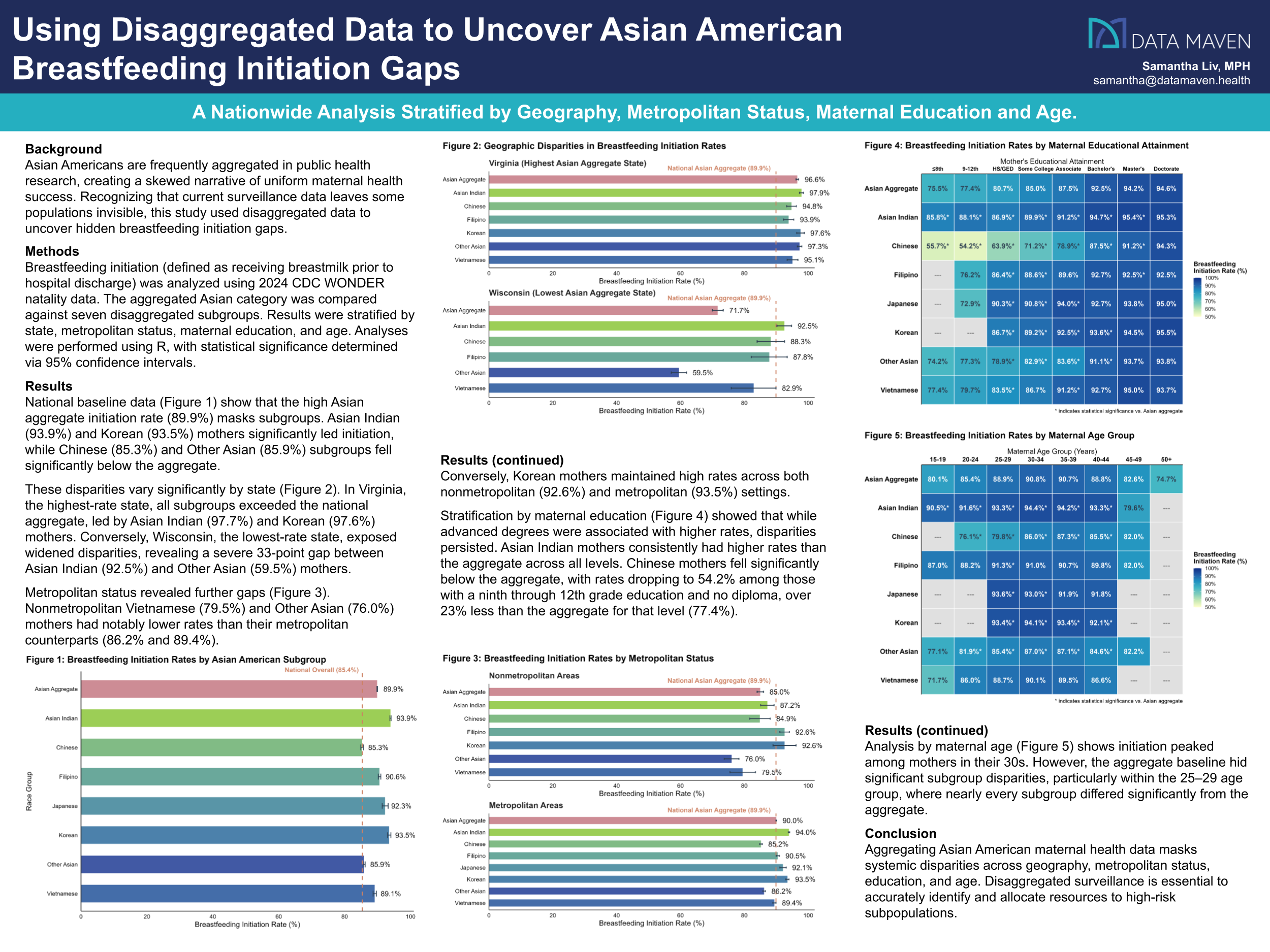
Asian Americans are frequently aggregated in public health research, creating a skewed narrative of uniform maternal health success. Recognizing that current surveillance data leaves some populations invisible, this study used disaggregated data to uncover hidden breastfeeding initiation gaps.
Methods
Breastfeeding initiation (defined as receiving breast milk prior to hospital discharge) was analyzed using 2024 CDC WONDER natality data. The aggregated Asian category was compared against seven disaggregated subgroups. Results were stratified by state, metropolitan status, maternal education, and age. Analyses were performed using R, with statistical significance determined via 95% confidence intervals.
Results
National baseline data show that the high Asian aggregate initiation rate (89.9%) masks subgroups. Asian Indian (93.9%) and Korean (93.5%) mothers significantly led initiation, while Chinese (85.3%) and Other Asian (85.9%) subgroups fell significantly below the aggregate.
These disparities vary significantly by state. In Virginia, the highest-rate state, all subgroups exceeded the national aggregate, led by Asian Indian (97.7%) and Korean (97.6%) mothers. Conversely, Wisconsin, the lowest-rate state, exposed widened disparities, revealing a severe 33-point gap between Asian Indian (92.5%) and Other Asian (59.5%) mothers.
Metropolitan status revealed further gaps. Nonmetropolitan Vietnamese (79.5%) and Other Asian (76.0%) mothers had notably lower rates than their metropolitan counterparts (86.2% and 89.4%). Conversely, Korean mothers maintained high rates across both nonmetropolitan (92.6%) and metropolitan (93.5%) settings.
Stratification by maternal education showed that while advanced degrees were associated with higher rates, disparities persisted. Asian Indian mothers consistently had higher rates than the aggregate across all levels. Chinese mothers fell significantly below the aggregate, with rates dropping to 54.2% among those with a ninth through 12th grade education and no diploma, over 23% less than the aggregate for that level (77.4%).
Analysis by maternal age shows initiation peaked among mothers in their 30s. However, the aggregate baseline hid significant subgroup disparities, particularly within the 25–29 age group, where nearly every subgroup differed significantly from the aggregate.
Conclusions and Public Health Impact
Aggregating Asian American maternal health data masks systemic disparities across geography, metropolitan status, education, and age. Disaggregated surveillance is essential to accurately identify and allocate resources to high-risk subpopulations.